Literature Sharing | Timing and Implementation Progress of Early Rehabilitation for Critically Ill Patients
This article is excerpted from: Xu Yan, Chen Dechang; "Chinese Critical Care Medicine" Volume 36, Issue 09, 2024 (excerpt)
I. Current Status of Critical Care Rehabilitation
During ICU treatment, in terms of the musculoskeletal system, immobilization can exacerbate the weakness or impairment of muscle function. Long-term disuse of the musculoskeletal system and increased overall catabolism can lead to muscle atrophy, muscle weakness, and joint stiffness and contracture. It may also result in osteopenia and osteoporosis. In terms of the nervous system, sleep rhythm disorders can cause cognitive dysfunction and even delirium in patients. In terms of the cardiovascular system, a decrease in cardiac output can lead to an increased resting heart rate, which in turn can cause cardiac dysfunction. In terms of the respiratory system, limited mobility, mechanical ventilation, and analgesic and sedative medications may cause a decrease in airway clearance ability, a reduction in tidal volume and functional residual capacity, diaphragmatic weakness, and decreased lung function. At the same time, reduced gastrointestinal motility, poor absorption, and atrophy of intestinal mucosa and glands can lead to malnutrition. It may also cause chronic inflammation, chronic anemia, deep vein thrombosis, etc.
Studies have shown that 50% to 70% of patients discharged from the ICU to rehabilitation centers exhibit impaired cognitive function, while 60% to 80% of patients display functional impairment or ICU-acquired weakness (ICU-AW). The lingering issues from critical illness persistently affect patients and their families. As the number of ICU survivors increases, the focus of ICU research should not only be on mortality rates, but also on the health-related quality of life of ICU patients.
Early rehabilitation can shorten ICU stay, prevent delirium, and improve patient prognosis. Implementing early rehabilitation in ICU patients is safe and feasible. For critically ill patients who receive vasoactive drug therapy, assisted mechanical ventilation, continuous renal replacement therapy, or even rely on extracorporeal membrane oxygenation support, the positive effects of early rehabilitation therapy significantly outweigh the potential risks.
II. The Dilemma of Early Rehabilitation
Currently, for critically ill patients with conditions such as acute myocardial infarction, pulmonary embolism, and skin grafting after extensive burns, the main treatment strategy remains focused on limiting activity to alleviate pain and protect cardiopulmonary function. However, some researchers have questioned the efficacy of this approach. In the future, when selecting treatment options for critically ill patients, emphasis will be placed on post-treatment function, with the goal of achieving maximum functional recovery for patients. However, due to the fact that physical movement can lead to increased cardiac output and oxygen consumption in ICU patients, resulting in physiological changes such as hypotension and hypoxemia, there are still many obstacles in controlling the timing of early rehabilitation intervention for critically ill patients. Furthermore, critically ill patients may have one or multiple organ dysfunction, requiring treatments such as mechanical ventilation, analgesia and sedation, and various vasoactive drugs during the treatment process. ICU patients are surrounded by numerous treatment and monitoring tubes, and changes in body position and limb movement during rehabilitation increase the safety risks associated with removing medical equipment. Therefore, when setting early rehabilitation exercise therapy goals, further attention and research should be given to the consideration of risk-benefit ratio. Although rehabilitation therapy for ICU patients should become a routine treatment method for critically ill patients, like analgesia and sedation, nutritional support, etc., early rehabilitation activities for critically ill patients are only safe, feasible, and effective under a multidisciplinary collaboration model in experienced centers.
Studies have shown that the average early mobility rate among ICU patients is 30.9%, with variations in early mobility rates among ICU patients influenced by factors such as different types of artificial airways, disease types, and whether they reside in developed countries. The implementation of early rehabilitation exercise for critically ill patients requires the guidance of a multidisciplinary team with experience and expertise, as well as the establishment of screening and safety protocols. Currently, in clinical practice, due to limitations in space, equipment, and human resources, ICU patients still face numerous challenges in undergoing early rehabilitation.
III. Practice of severe disease rehabilitation
1. Assessment of rehabilitation needs: For patients admitted to the ICU for more than 1 day, a systematic assessment of their rehabilitation needs should be conducted. The standardized evaluation and recording of patients' rehabilitation status is a key step in developing initial rehabilitation plans for the ICU. Currently, the commonly used scales for assessing the rehabilitation status of ICU patients mainly include the Functional Status Score for ICU (FSS-ICU), the ICU Mobility Scale (IMS), and the Surgical Optimal Mobility Score (SOMS).
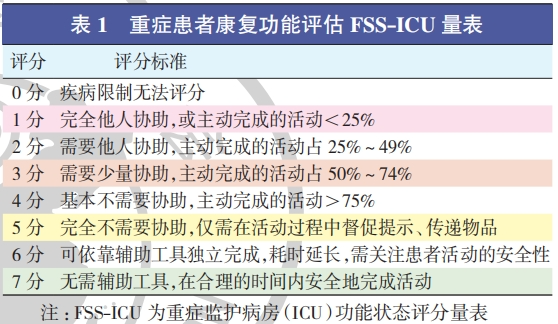
① Functional Status Score for ICU (FSS-ICU)

②. ICU Mobility Scale (IMS)
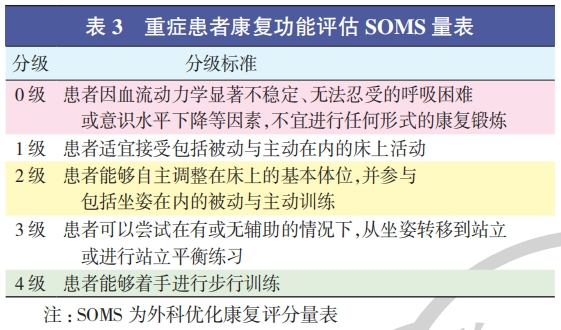
③. Surgical Optimal Mobility Score (SOMS)
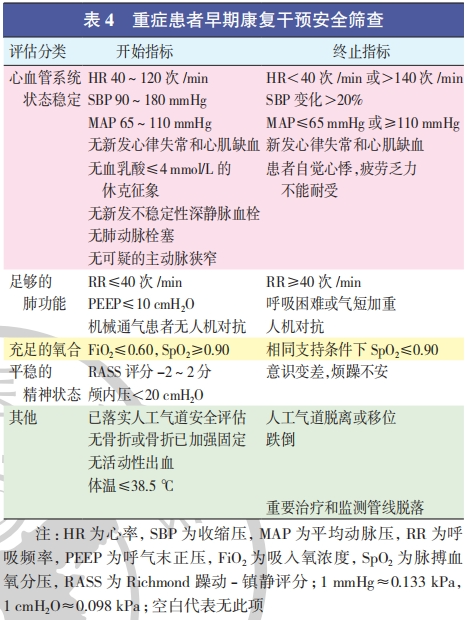
2. Timing of rehabilitation intervention: Although rehabilitation therapy should be initiated as early as possible after assessing the patient's rehabilitation needs and provided that the patient's condition permits, critically ill patients are characterized by severe and rapidly changing conditions. Comprehensive consideration of the diagnosis and treatment plan is the foundation for promoting the smooth progress of treatment. Currently, the safety of exercise is comprehensively considered from aspects such as the respiratory system, circulatory system, nervous system, major internal and surgical diseases, and patient complaints, serving as the evaluation criteria for the initiation and termination of exercise intervention. Chinese scholars have also summarized safety standards, ultimately forming a safety screening for early rehabilitation intervention in severe diseases (Table 4) that provides content reference and quantitative standards, with the aim of providing a basis for the timing of initiation and termination of early rehabilitation for severe diseases.
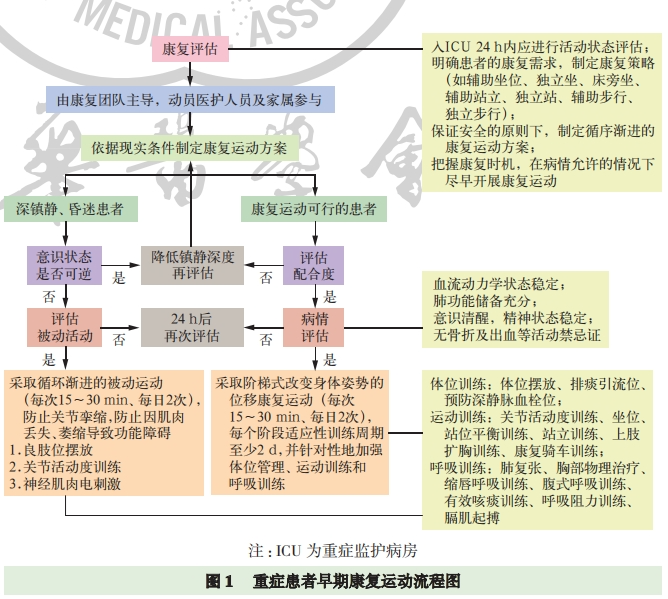
3. Implementation Process: Individualized treatment for critically ill patients is based on principles such as "goals and objectives", "continuity and dynamism", and "treatment and re-injury". Comprehensive consideration of the diagnosis and treatment plan is the foundation for smoothly advancing treatment. Senior physicians, case discussions, and multi-disciplinary treatment (MDT) discussions can provide predictive judgments, develop individualized rehabilitation treatment strategies, and control the overall condition, as well as macro and specific treatment plans. Based on the existing evidence, a flowchart for early rehabilitation exercise for critically ill patients (Figure 1) involving multidisciplinary participation is summarized, including rehabilitation exercise programs, key steps of rehabilitation training, and monitoring and evaluation of the rehabilitation process.
4. Treatment methods
① Posture training:
For patients in a persistent coma, rehabilitation strategies should primarily focus on preventing complications, such as pressure ulcers, joint contractures, spasms, pulmonary infections, and deep vein thrombosis. Measures such as changing body position and passive joint mobilization should be taken.
Neuromuscular electrical stimulation (NMES) is commonly used for patients who are unable to participate in activities. By stimulating nerve fibers to activate motor neurons, it increases muscle blood flow and contractility, promotes muscle microcirculation, delays muscle atrophy, and improves muscle strength and endurance. It is also used to prevent ICU-acquired weakness (ICU-AW) in critically ill patients.
For patients who can cooperate with rehabilitation therapy but whose condition is unstable and unsuitable for immediate implementation, although exercise training cannot be performed, it is still necessary to protect the joint functional position. When muscle tension is high, the patient should be placed in an extended position to prevent contracture;
During positional drainage, the patient's position should be adjusted according to the course of each pulmonary segment bronchus, so that the diseased segment bronchus is perpendicular to the main bronchus. By utilizing the gravitational force, combined with methods such as percussion and vibration, secretions can be loosened and moved to the airway. Patients are assisted in expectorating sputum through coughing or artificial secretion removal techniques②Sports Training:
For ICU patients who are stable and cooperative, a strategy of "low starting point, slow increase" can be adopted. Initially, manual therapy can be used to increase joint mobility training, with emphasis on neck and trunk mobility training. At the same time, mobilization therapy can be performed on the joints and small joints of the shoulder, elbow, wrist, fingers of the upper limbs, and hip, knee, ankle of the lower limbs.
Furthermore, rehabilitation training for the upper and lower limbs can be implemented based on the patient's range of joint motion. Passive training should be carried out first, and then active training can be performed once the limb mobility has improved, gradually improving limb function. Exercise for upper and lower limb mobility can stimulate the reorganization of motor cortex function, thereby improving limb dysfunction, facilitating the restoration of reactive balance control, and enhancing balance function.
③ Respiratory training:
Respiratory function training focuses on the lungs and respiratory tract, and is closely related to overall rehabilitation training. It includes postural drainage, chest physical therapy, abdominal breathing training, pursed lip breathing training, effective expectoration training, respiratory resistance training, etc.
For patients with spontaneous breathing, abdominal breathing training is the basic mode of respiratory rehabilitation, which should be combined with pursed lip breathing technique, cough and expectoration technique, active cycle breathing technique, etc.
For patients undergoing mechanical ventilation in the acute and subacute phases, the main contradiction in the respiratory system may not be the weakness of inspiratory muscles. Implementing lung and diaphragm protective ventilation is the key to treatment at this time. Specifically, priority should be given to lung protective ventilation strategies (lung rest ventilation strategies) to reduce excessive lung stress, strain, and stress accumulation, while maintaining appropriate inspiratory effort and diaphragm protective ventilation strategies that ensure expiratory synchrony. This approach can improve patient prognosis, alleviate dyspnea, prevent complications, reduce mortality, and enhance patient functional status and quality of life.
Inspiratory muscle training (IMT) can shorten the duration of mechanical ventilation and improve ventilator dependency. IMT employs a "high-intensity, low-repetition" strategy. For patients with mechanical ventilation duration >7 days, breathing through a spring respiratory resistance trainer, which increases resistance during inhalation, aims to maximize the stimulation of inspiratory muscle movement.
External diaphragmatic pacing is a relatively advanced method for assisting diaphragmatic rehabilitation therapy. The diaphragm is the main inspiratory muscle, and the phrenic nerve controls diaphragmatic movement to maintain normal ventilation function. By stimulating the phrenic nerve through surface electrodes to induce diaphragmatic contraction, respiratory function can be improved and the muscle strength of the patient's respiratory muscles can be enhanced. However, precise positioning of the electrodes is difficult, the therapeutic effect varies greatly, and improper operation can easily cause diaphragmatic fatigue. Moreover, most current studies assess the impact on diaphragmatic dysfunction indirectly, lacking more reliable data. Further exploration is needed to evaluate the potential physiological mechanisms of diaphragmatic pacing and the optimal treatment parameters and evidence.
5. Early rehabilitation exercise monitoring:
Overall monitoring based on the patient's condition is an integral part of early rehabilitation therapy. For example, rehabilitation exercise should be delayed in severe shock states. After the shock is under control, rehabilitation exercise assessment can be initiated as soon as possible, while being vigilant for signs such as hypotension and hypoxemia.
For patients undergoing extracorporeal membrane oxygenation (ECMO) support, it is even more crucial to closely monitor and dynamically adjust the ECMO and mechanical ventilation parameters to ensure adequate oxygen supply to the patient.
The rehabilitation treatment for critically ill patients requires monitoring the disease progression, hemodynamic treatment intensity, and the oxygen supply and demand metabolic status of tissues and organs to develop optimal early rehabilitation strategies. During the rehabilitation exercise, if there are situations such as high pressure alarms from infusion devices, increased injection resistance of push syringes, or fluid leakage from pipeline connections in the treatment and monitoring pipelines that cannot be paused, empirical treatment or replacement should be promptly implemented.
Effective diagnosis and treatment of the primary disease, adequate analgesia, assessment of delirium, psychological support therapy, and proper tube assessment are comprehensive management strategies to prevent adverse events of tube detachment.
Once clinical manifestations specified in the safety screening termination criteria for early rehabilitation intervention in severe patients are observed, namely symptoms of cardiopulmonary dysfunction and myocardial infarction, intolerable dyspnea, and manifestations of deterioration in other systems' functions, rehabilitation exercise must be immediately stopped.
IV. Comprehensive Solution for Early Rehabilitation by the Bedside for Patients
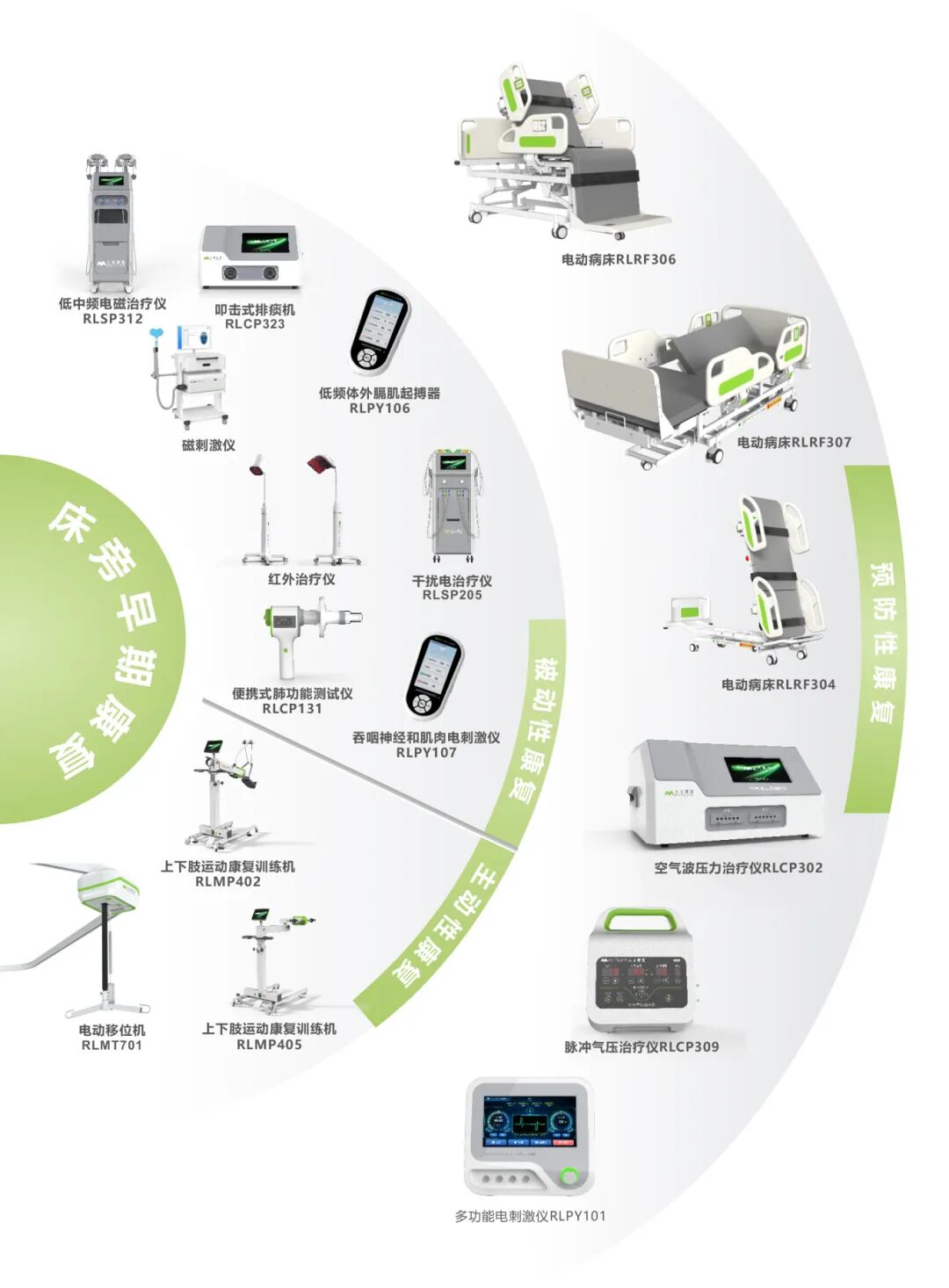
Retlife Fangfu has launched a bedside early rehabilitation solution, providing integrated services for the construction of full-cycle early rehabilitation to hospitals at all levels across the country.

Preventive rehabilitation: Interventions are carried out through scientific means to avoid or delay the occurrence of functional impairment, thereby improving long-term quality of life and independent living ability.
Passive rehabilitation: Rehabilitation activities are carried out by medical staff or rehabilitation therapists with the aid of external forces when patients have no active movement ability at all (such as deep sedation, coma, or extreme weakness).
Active rehabilitation: Active rehabilitation refers to rehabilitation training that is completed by patients themselves under the guidance and supervision of medical staff or therapists, after they have clear consciousness, relatively stable vital signs, and a certain ability to follow instructions and exert force actively. This is a key step towards achieving substantial functional recovery.









